
Case #23
-
History: 22 year old male dove into a shallow pool. Presents with quadriplegia and suspected anterior cord syndrome.
© 2012 Must See Radiology
History: 22 year old male dove into a shallow pool. Presents with quadriplegia and suspected anterior cord syndrome.
© 2012 Must See Radiology


Axial and sagittal CT images of the cervical spine
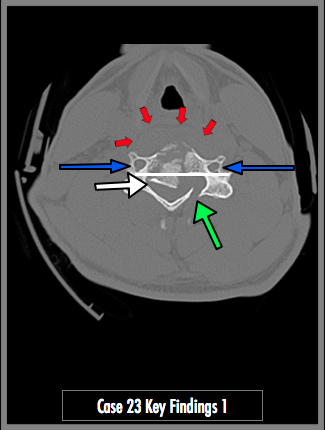
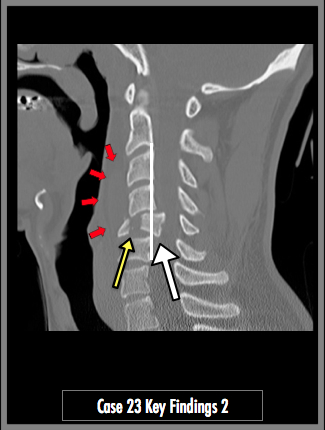
Complete coronal plane comminuted fracture through the C5 vertebral body (yellow arrow). There is retropulsion (abnormal posterior movement of the vertebral body representing disruption of the posterior longitudinal ligament, white line) of the vertebral body into the central spinal canal (white arrow). The fractured anterior-inferior corner of the vertebral body appears as a 'teardrop'. There is associated prevertebral soft tissue hematoma (red arrows). There is an additional fracture through the left lamina of C5 (green arrow). It is important to note the vertebral artery foramen are not fractured (blue arrows). See additional findings below.
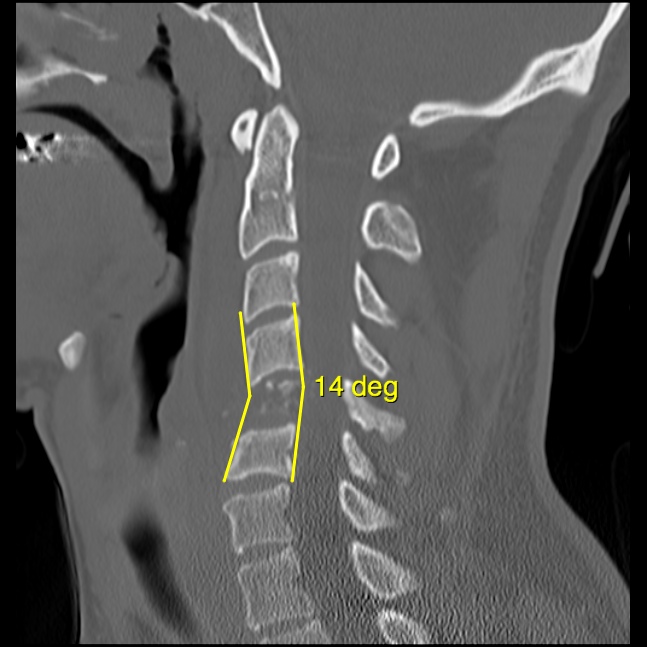
The axial-flexion injury resulted in cervical kyphosis of approximately 14 degrees. Cervical kyphosis of more than 10 degrees in adult patients (20 deg in children) alone suggest surgical fixation. Also note the near total absence of the C5 vertebral body at this sagittal slice. This appearance represents a sagittally oriented fracture, better demonstrated on the coronal view below.
The anterior-inferior fracture fragment resembles a falling tear drop, hence the name "tear drop fracture". This fracture is most common at C5 in patients sustaining flexion axial-load injuries from diving and motor vehicle crashes. The teardrop fragment typically remains align with the vertebral body below it. It may also show some downward and anterior displacement compared to the inferior vertebral body, as it does in this case.
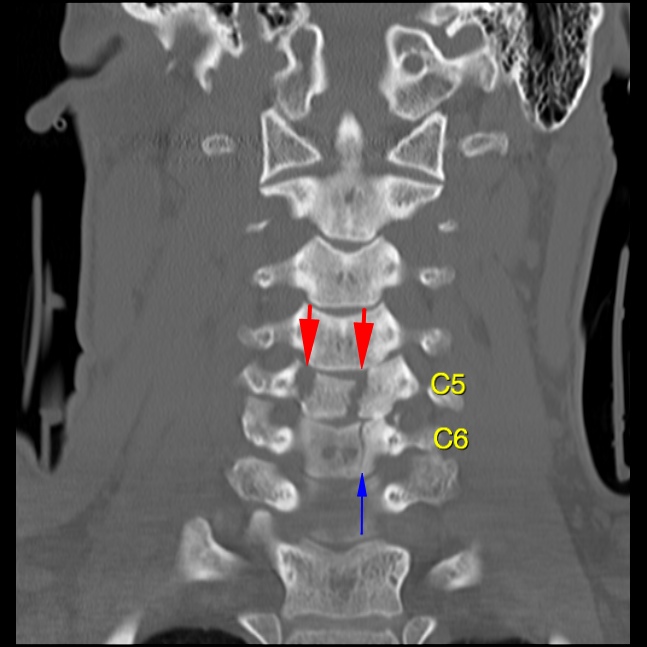
The large red arrows are directed towards two sagittal fractures through the C5 vertebral body. Careful examination of the coronal images reveals a second fracture through the C6 vertebral body. This sagittal fracture extends through the entire vertebral body and posterior left elements. It is also seen well on the axial images (not shown here). This fracture is also a classic appearance for a flexion axial load injury to the cervical spine. This appearance may be present by itself in a much less severe case. A presentation of anterior cord syndrome with no obvious radiographic findings may suggest this type of fracture and careful examination of the CT in the lower cervical spine is required.
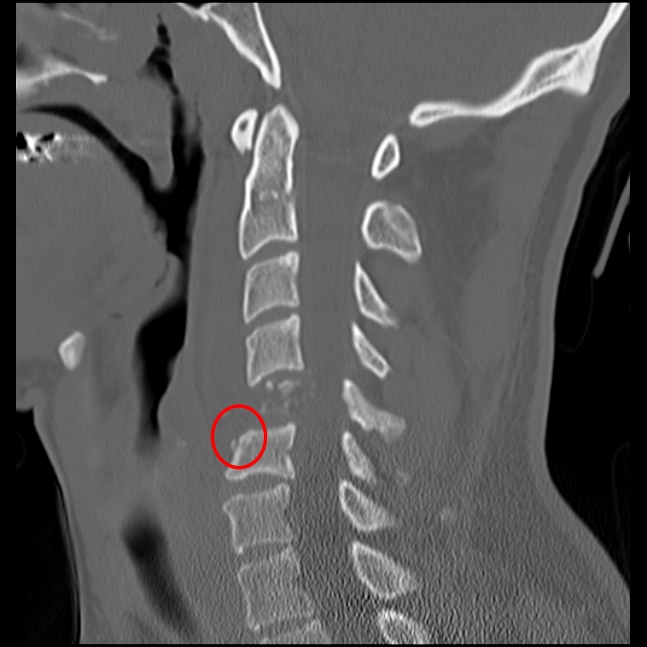
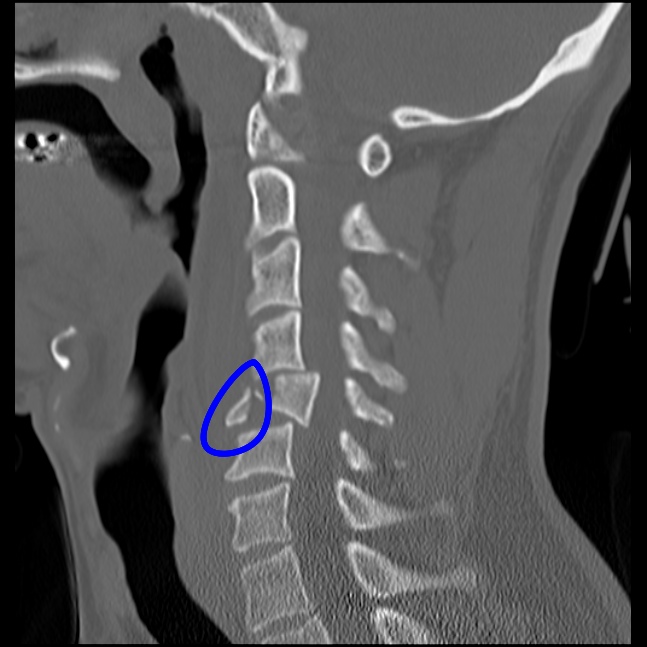
Another diagnostic finding that represents flexion axial-load injury is a anterior-superior endplate minimal compression deformity with fracture (red circle).
© 2012 Must See Radiology
C5 Burst / Flexion-Teardrop Fractures
& C6 Burst Fracture
This case demonstrates characteristics of both axial compression and hyper flexion injuries. The fracture at C5 demonstrates components of both, while the fracture at C6 is more of an axial compression fracture. Here are characteristics of both:
Flexion Teardrop Fracture:
- HYPERFLEXION INJURY
- Most severe and unstable injury of C-spine
- Anterior-inferior fracture fragment alignment is closer to vertebral body below fracture.
- Remaining posterior fracture fragment may be aligned with more superior vertebral body.
- Coronal oriented fractures
- All ligaments are disrupted
- Kyphosis
- Usually located at C5-C6
- Severe compromise of spinal canal due to retropulsion of body
Burst Fracture:
- AXIAL COMPRESSION INJURY
- May be a stable fracture if isolated compression
- Comminuted fracture of the centrum from the intervertebral disk ramming into it
- Ligaments usually maintained
- Neurologic deficit in ~85% patients due to retropulsed bone fragments
- Usually located at C5-C7
- Fracture plane is in the sagittal plane (vertically oriented through the whole vertebral body in the AP plane)
- Minimal compression fracture of the anterior superior endplate may be present
- Similar in mechanism to Jefferson Fracture (C1-C1 axial compression fracture)
- May be subtle and not immediately identified on cervical spine radiographs.
A nice breakdown of these fractures is in Dahnert's text (ref below).
Additional Information:
Torg, JS. "The axial load teardrop fracture. A biomechanical, clinical and roentgenographic analysis." Am J Sports Med July 1991: 19(4), 355-64.
© 2012 Must See Radiology
Not available at this time.
Rating not available at this time.
Any feedback regarding this case can be emailed to Tony@mustseeradiology.com
Thank you for trying Must See Radiology!
© 2012 Must See Radiology